Answer to Mid-Month Mindbender
Prurigo pigmentosa
The disease was first described by Nagashima in Japan in 1971. It is characterised by intensely itchy papulovesicles on the trunk and heals with net-like pigmentation. Histologically, it is characterised by a dense superficial dermal infiltrate of neutrophils that ascend to the epidermis and form abscesses. There is also accompanying spongiosis and ballooning. Later lesions contain dermal melanophages. The important differential diagnosis is dermatitis herpetiformis, in which the neutrophils are confined to the tips of dermal papillae and do not involve the epidermis.
Fox-Fordyce disease or Apocrine Miliaria
Foamy histiocytes within the dermis are seen in diverse conditions such as xanthomas, xanthogranulomas and lepromatous leprosy. However, the presence of foamy histiocytes preferentially around dilated infundibula is seen only in Fox-Fordyce disease. Spongiosis is also seen in the infundibulum. Cornoid lamellae, deemed to be characteristic of porokeratosis, can also be seen in this condition.
Anti laminin gamma 1, seen in anti laminin gamma 1/anti p200 pemphigoid
Anti laminin gamma 1 has been identified as the target antigen in the rare variant of bullous pemphigoid (BP), called anti Laminin gamma 1 or anti-p200 pemphigoid. Classic pemphigoid is characterised by antibodies to BP 180 and 230, which show up as IgG and C3 deposits in a basement membrane zone (BMZ) pattern and localise to the roof of the blister on indirect IF. In contrast, anti-p200 pemphigoid binds to the floor of the split, similar to epidermolysis bullosa acquisita and may be mislabelled as such. Distinction of these two diseases requires immunoblotting. Anti LAD1 is responsible for linear IgA disease.
Trichoepithelioma and Basal cell carcinoma
Both trichoepithelioma and basal cell carcinoma (BCC) show trichoblastic i.e. hair follicle differentiation; the former being benign and the latter, malignant. It is difficult to differentiate the two based on morphology alone, the problem being magnified in distinguishing desmoplastic trichoepithelioma from morphea-like BCC.
Cytokeratin 20 is a marker for Merkel cells, which are normally present in the basal layers of the epidermis and hair follicles. It has been demonstrated that CK 20 positive cells are seen in benign tumors with trichoblastic differentiation and not in malignant ones. Androgen receptor expression is seen in most BCCs, but not in trichoepitheliomas. CD10 shows stromal reactivity in trichoepitheliomas, highlighting the “germ and papilla” structures, which are diagnostic. In BCC, CD10 is expressed only by the neoplastic cells.
In summary, cytokeratin 20, CD10 and androgen receptors are useful in distinguishing between benign and malignant trichoblastic tumors.
Wiry collagen in the papillary dermis
Normal basket-woven orthokeratosis, dermal oedema and extravasated RBCs are signs of acuteness in a lesion. Necrotic keratinocytes are usually abundant and may be seen at all levels of the epidermis. These are usually accompanied by extensive vacuolar interface dermatitis, the commonest histopathologic pattern of a drug eruption.
Wiry collagen bundles in the papillary dermis are often seen in mycosis fungoides, pityriasis lichenoides chronica and lichenoid purpura. These are seen along with a lichenoid infiltrate of lymphocytes and reflect the long-standing nature of the process.
Drug eruptions can display a multitude of histopathologic patterns. When one encounters several patterns within a single biopsy specimen or features that do not correspond to any known disease, it is reasonable to assume that the culprit is a drug and proceed accordingly.
Atrophie blanche
Atrophie blanche represents healed lesions of livedo vasculitis. The remaining three are expressions of leucocytoclastic vasculitis (LCV).
Fully developed LCV is diagnosed on histopathology on the basis of fibrin in vessel walls with or without thrombi, perivascular infiltrates and nuclear dust.
Henoch-Schonlein purpura is LCV with deposits of IgA in the vessels, usually seen in children. Extracutaneous manifestations are frequent, in the form of abdominal pain, haematuria and joint pains. Finkelstein’s disease, also known as acute haemorrhagic edema of infancy , is LCV that presents as purpuric lesions/plaques on the face and extremities of infants. Granuloma faciale presents as plaques/nodules on the face. Microscopically, it shows LCV with extensive dermal fibrosis, often in a storiform fashion and is not a granulomatous disorder. Erythema elevatum diutinum is its twin in a different anatomic location, the extremities.
Atrophie blanche is typified by depressed white scars on the legs, which represents healed livedo vasculitis. Livedo vasculitis is characterised by fibrin and thrombi often in the same vessel and accompanying lymphocytic infiltrates. Infarction and necrosis of the epidermis occur and finally lead to sclerosis and loss of pigmentation.
Bananas
In ochronosis, both alkaptonuria and acquired, the ochronotic pigment on H & E staining takes up an ochre colour. It is found deposited within collagen bundles causing homogenisation and swelling of the collagen bundles, an appearance referred to as 'banana figures' or 'banana shaped bodies'.
The short hyphae and clusters of the yeast form of the Malassezia species on microscopy is called 'banana and grapes', more often referred to as 'spaghetti and meat ball' appearance.
The elongated nests of nevus cells in a Spitz nevus are sometimes found to hang down the rete ridges giving it an appearance of 'hanging bananas' or 'bunches of bananas'!
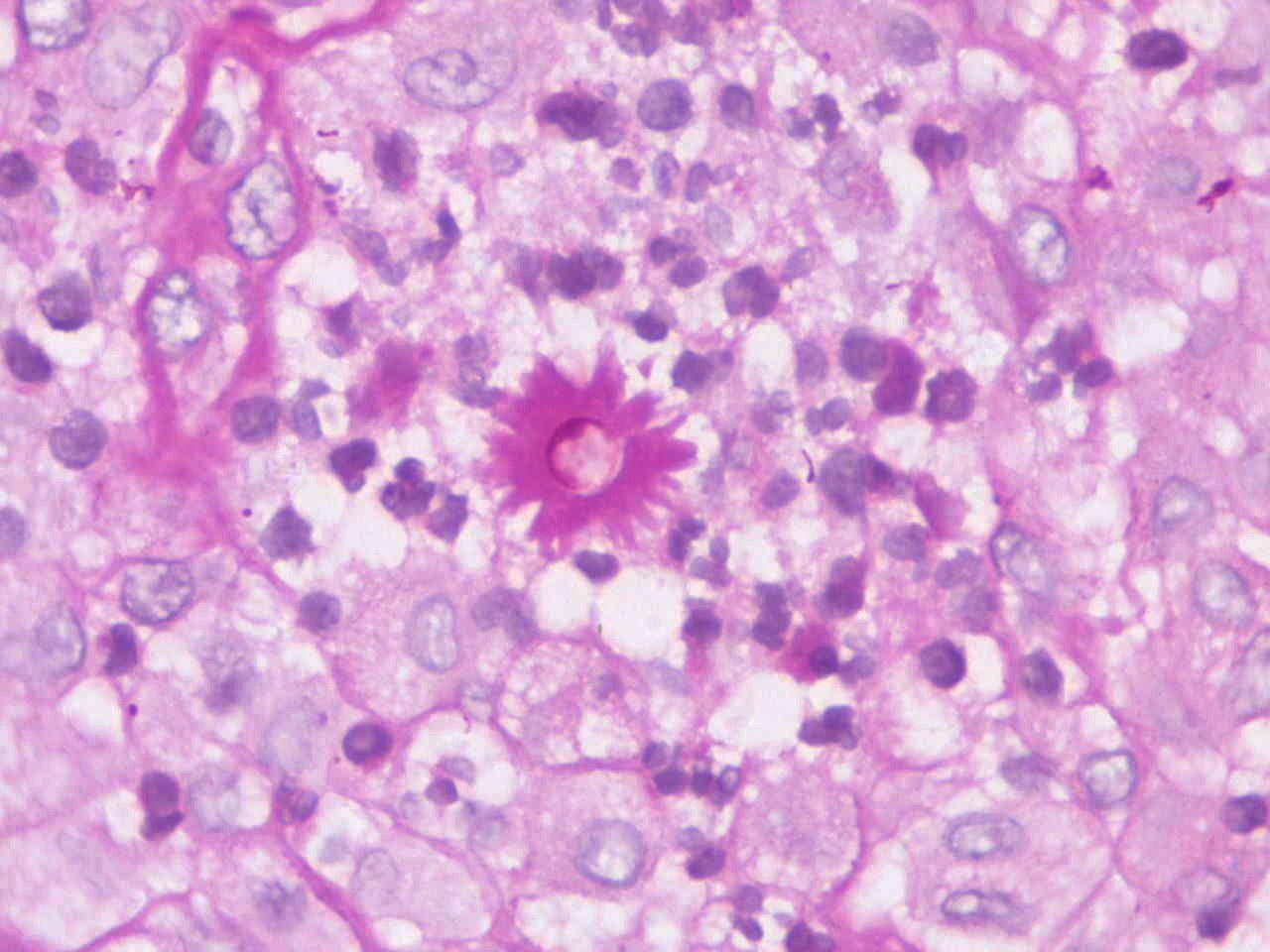
Sporothrix schenckii
This etiological agent of sporotrichosis (rose-pickers disease) is a dimorphic fungus. It clinically presents in 3 main ways: localized/fixed, lymphangitic/sporotrichoid and disseminated/systemic disease with the sporotrichoid presentation being most common. In the localized variant, several types of granulomas (tuberculoid, histiocytic, suppurative) may be found in the dermis. Cigar bodies represent the elongated yeast like form of the fungus and when these yeast forms are surrounded by eosinophilic hyaline ray like processes they are referred to as ‘sporothrix asteroid’ (see image), usually seen in the centre of suppurative granulomas.
{kind=link}
Necrobiotic xanthogranuloma
All the above mentioned conditions are collagenolytic (necrobiotic) granulomas which may be classified into 'blue' granulomas where the necrobiotic area stains basophilic due to the presence of mucin and 'red' granulomas which stain eosinophilic due to the presence of fibrin, eosinophils and flame figures. 'Blue' granulomas include granuloma annulare, Wegeners granulomatosis and rheumatoid vasculitis while 'red' granulomas include necrobiosis lipoidica, rheumatoid nodule, pseudorheumatoid nodules, necrobiotic xanthogranuloma, Wells syndrome and Churg Strauss syndrome.
Necrotic keratinocytes
Last week’s sign refers to a fading dermatosis, a dermatosis no longer active but was presumably so, a few days earlier. The feature that does not fit in is the presence of numerous necrotic keratinocytes.
Chanarin Dorfman syndrome (Neutral lipid storage disease)
This autosomal recessive condition occurs due to the inability to breakdown endogenous triglycerides resulting in its consequent accumulation in various tissues and organs. It is characterized by ichthyosis which usually manifests at birth as a collodion baby or erythroderma, along with other systemic features such as hepatosplenomegaly, myopathy, cataracts and deafness.
A typical feature on light microscopy is the presence of lipid droplets in circulating polymorphs and monocytes (Jordans anomaly). Similar lipid droplets are also encountered in biopsies of the muscle and liver. Jordans anomaly may also be seen in Refsums disease, another ichthyotic disorder, however peripheral nerve thickening is a characteristic feature in the latter. Treatment includes emollients, systemic retinoids and possibly dietary restriction of long chain fatty acids.
Equine melanoma/ Animal-type melanoma/ Pigmented epithelioid melanocytoma
This is a rare variant of malignant melanoma initially described in gray horses. Clinically, it presents as a well-circumscribed bluish-black nodule or plaque, predominantly located on the scalp and the limbs. Satellite lesions are relatively common. It generally appears de novo. Mortality rates are lower than other melanomas though several instances of nodal and distant metastasis have been reported.
Histologic features include heavily pigmented dendritic and epithelioid cells occupying the full thickness of the dermis and occasionally extending into the subcutis with infiltration of adnexal structures. Histological differentials include nodular melanoma, malignant blue nevus, deep penetrating nevus and metastatic melanoma.
Jadassohn
The 'name' common to the 3 histological descriptions is 'Jadassohn'. Joseph Jadassohn was a noted German dermatologist and a pioneer in allergology. Several diseases/ entities have been named eponymously after him.
1. Borst-Jadassohn phenomenon is a histological pattern characterized by sharply defined intraepidermal nests of basaloid to epithelioid cells seen in conditions such as clonal seborrheic keratosis, actinic keratosis, Bowen's disease and hidroacanthoma simplex.
2. Jadassohn -Tieche nevus, another name for a common blue nevus, is histologically characterized by collection of bipolar and dendritic melanocytes in the interstices of dermal collagen, tending to concentrate around appendages and neurovascular bundles.
3. Jadassohn Pellizzari type of anetoderma is a variant of primary idiopathic anetoderma where the anetoderma is preceded by inflammatory changes in contrast to the Schweninger-Buzzi type which has a non-inflammatory onset. This classification though, is only of historical interest.
a)Malakoplakia
b)Von Hansemann cells
Malakoplakia is a chronic inflammatory disorder predominantly affecting the urogenital tract with the skin (vulva and perianal region) being rarely involved. It is mainly seen in the setting of immunosuppression and is believed to be due to defective phagolysosomal activity of macrophages resulting in an inadequate intracellular destruction of phagocytosed bacteria, particularly E.coli. Cutaneous lesions may show varied manifestation: papules, plaques, nodules, abscesses, fistulae, ulcers and polypoid masses.
Histologically, it is characterized by sheets of closely packed macrophages (Von Hansemann cells) which have a foamy cytoplasm and an eccentric rounded hyperchromatic nucleus. Michaelis-Gutmann bodies refer to the basophilic, concentric laminated inclusions within some of these macrophages. These cells stain positive with PAS, iron and calcium stains. Scattered lymphocytes and plasma cells are also seen.
Pancreatic panniculitis
All the conditions listed (subcutaneous fat necrosis of the newborn, sclerema neonatorum, post-steroid panniculitis and pancreatic panniculitis) histogically present as lobular panniculitis. However, all of these with the exception of pancreatic panniculitis are associated with deposition of needle shaped crystals within adipocytes which appear as radially arranged clefts. Pancreatic or enzymic panniculitis is characterized by necrosis within fat lobules of the panniculus resulting in 'ghosts' of lipocytes, a granulomatous infiltrate with Langhans giant cells and calcification.
Aquagenic palmoplantar keratoderma
Aquagenic palmoplantar keratoderma (transient aquagenic hyperwrinkling/ aquagenic syringeal acrokeratoderma) is predominantly an acquired sporadic condition which mainly affects adolescents and females. It may also be associated with cystic fibrosis.
Clinically it is characterized by edema with wrinkling of the palms and soles, pruritus and whitish papules on contact with water (hand in bucket sign). The most opportune time for a biopsy is after contact with water as there are no pathological changes when the biopsy is taken from dry lesion-free skin.
Histologically, it may appear as an invisible dermatosis but careful scrutiny reveals ortho-hyperkeratosis with acanthosis and spongiosis. A rather consistent finding is the dilatation of eccrine acrosyringia.
Tadpole is the common descriptive term
In 1983, Pariser reported the usefulness of a Tzanck smear in the diagnosis of spongiotic vesicular dermatitis and concluded that the presence of at least 10 epidermal cells having a 'tadpole' like shape per x100 field was a reliable marker of in this condition.
The cell of origin of a rhabdomyosarcoma, the rhabdomyoblast has an eosinophilic granular cytoplasm and may at times be elongated, hence the name strap cells or tadpole cells.
Tadpole shaped cells are also described in squamous cell carcinoma of the cervix and are also found in an unstained urinary sediment in squamous cell carcinoma of the bladder.
In syringomas, the ductal structures at times have comma-like tails giving them a 'tadpole' configuration.
Microcystic adnexal carcinoma (MAC)
MAC, also referred to as malignant syringoma, sclerosing sweat duct carcinoma and sweat gland tumor with syringomatous features is a locally aggressive malignant sweat gland tumor with a predilection for the head and neck region, particularly the central face and upper lip.
Histologically, the tumor is poorly circumscribed occupying the dermis and subcutis and on occasion may invade deeper tissue. The superficial part is composed of keratocysts and small squamoid and basaloid nests with variable ductal differentiation. A typical finding is diminution in the size of nests and cysts in the deeper part of the tumor. Perineural invasion is common, which is not a feature in syringomas. Eosinophils are present particularly in areas of lesional clear cell change.
CD5 helps to differentiate MAC from morphea-like basal cell carcinomas and desmoplastic trichoepithelioma. CK-15 and CK-7, also positive in desmoplastic trichoepitheliomas, are negative in infiltrative basal cell carcinomas and squamous cell carcinomas.
Pearly penile papules
These are angiofibromas.
The other four choices have a link to the sebaceous gland.
Fordyce spots or Fordyce granules are ectopic sebaceous glands found in the vermilion border of the lips, cheeks, the glans or the vulva.
Muir-Torre syndrome is an autosomal dominant hereditary non-polyposis colorectal cancer syndrome associated with neoplasms of the skin, the most common being sebaceous tumours such as sebaceous carcinoma.
Juxtaclavicular beaded lines is an asymptomatic papular eruption over the neck and supraclavicular region characterized histologically by sebaceous gland hyperplasia in the immediate subepidermal zone.
Steatocystoma multiplex are multiple sebum containing dermal cysts, the walls of these cysts containing embedded lobules of sebaceous glands.
Mulberry or morula
All the conditions mentioned above are characterized by 'mulberry' or 'morula' cells.
Hibernoma is a benign tumor consisting of adipocytes that resemble normal brown fat. Microscopically, it is characterized by large fat cells with a multivacuolated granular eosinophilic cytoplasm giving rise to the name 'mulberry', 'morula' or ping pong' cells
Protothecosis is a rare infection caused by the genus Prototheca, an achlorophyllic ubiquitous algae which is known to cause cutaneous lesions, disseminated or systemic disease and olecranon bursitis. On histology, dermal sporangia with endosporulation/(mulberry appearance) is seen, better demostrated with fungal stains like PAS and GMS. A typical feature of this endosporulation is the presence of a central round endospore with a corona of moulded endospores.
Fabry's disease is an X-linked lysosomal storage disorder characterized by excessive deposition of neutral glycosphingolipids in vascular endothelium of various organs, epithelial cells and smooth muscle cells. 'Mulberry' cells are fat laden epithelial cells and can be seen in urinary sediment of such patients. Mulberry like figures are also seen on electron microscopy in the eccrine glands.
Multinucleated giant cells (Warthin Finkeldy or mulberry cells) are seen in hyperplastic lymphoid tissue (lymph nodes, tonsils, adenoids, spleen, appendix and thymus in the prodromal phase of measles.
Focal epithelial hyperplasia or Heck disease
Focal epithelial hyperplasia or Heck disease is an uncommon viral proliferation (HPV 13 and 32) of the oral mucosa encountered mainly in Eskimos (Inuits) and Native Americans.
It is usually seen in children or young adults and clinically manifests as multiple pink or whitish papules or nodules in the oral mucosa. The diagnostic histologic appearance is the 'bronze age battle axe' appearance which is an abrupt and considerable focal acanthosis with clubbing and occasional anastamosis of the rete ridges. Another feature is the presence of 'mitosoid' cells or cells resembling those in various phases of mitosis, though they actually lack mitotic ability. These are degenerating epithelial cells with irregular hyperchromatic nuclei found in clusters in the upper stratum spinosum.
Paracoccidiodomycosis/ South American Blastomycosis/ Lutz-Splendore-de-Almeida disease
Paracoccidiodomycosis is a systemic mycosis, endemic to South and Central America, caused by the dimorphic fungus Paracocciodes brasiliensis. The fungus is a saprophyte and the portal of entry is usually the respiratory tract. Direct man to man transmission does not occur.
The less common acute or subacute forms manifest as fever with constitutional symptoms, skin lesions, lymphadenopathy and hepatosplenomegaly. The more common chronic or adult form presents with pulmonary features (cough, dyspnoea, fibrosis, bullae and emphysematous changes), oropharyngeal and laryngeal mucosal involvement (typical presentation being erythematous ulcers with a granulomatous base intermixed with hemorrhagic spots, the so called moriform stomatitis of Aguiar-Pupo), polymorphic cutaneous lesions (crusted papules, ulcers, verrucous plaques and nodules) and lymphadenopathy.
The histopathological findings include pseudoepitheliomatous hyperplasia with intraepithelial abscesses and epithelioid granulomas with foci of suppuration.
The hallmark feature is the presence of round, large and small budding yeast cells which often demonstrate multi-lateral budding giving it the typical mariners or pilots 'steering wheel' appearance. These may be found within macrophages and foreign body giant cells or lying free in tissue and are more easily demonstrable using silver stains.
Paisley tie
'Paisley' pattern, a droplet shaped vegetable motif of Persian origin is a popular design on various jewelry and textiles including ties. A 'paisley tie' or 'tadpole' appearance in dermatopathology is encountered in syringoma, microcystic adnexal carcinoma, morpheaform basal cell carcinoma and desmoplastic trichoepithelioma to describe the configuration of tumor cell nests.
The other options are descriptive terms for a pattern of keratinization seen in adnexal cysts of pilo-sebaceous origin.
'Sharks tooth' cuticle is the wavy eosinophilic crenulated appearance of the cyst wall in steatocystoma multiplex. 'Rolls and scrolls' is seen in a proliferating pilar cyst, as the epithelium proliferates, the wall buckles inward rolling on itself producing a trabecular or scroll like appearance. 'Onion skin' is the stratified lamellated appearance of corneocytes in the lumen of epidermoid and vellus cysts.
Renal medullary carcinoma
Multiple cutaneous neoplasms characterised by fenestrate pattern of mantle-like cells surrounded by ribbon like collagen bundles (fibrofolliculoma) with clusters of sebocytes at times (trichodiscoma, a variant) are seen in Birt-Hogg-Dube syndrome. It is a rare disease, associated with lung cysts and increased predisposition to develop renal tumors. The common renal neoplasms seen are chromophobe renal cell carcinoma, oncocytoma and rarely clear cell carcinoma, papillary carcinoma. There may also be tumors in other organs like thyroid and the gastrointestinal tract. The disease occurs as a consequence of mutations in the folliculin gene.
Renal medullary carcinoma is a rare, aggressive neoplasm classically seen in patients with sickle cell disease.
Chronic atypical neutrophilic dermatosis with lipodystrophy and elevated temperature syndrome (CANDLE syndrome)
CANDLE syndrome is a rare autosomal recessive autoinflammatory disease which occurs due to a mutation in the PSMB8 gene leading to a dysregulation of the interferon signalling pathway. It presents in early infancy with recurrent fever and physical growth retardation. Patients have a typical facies: thick lips, violaceous swollen eyelids and facial lipodystrophy. Skin lesions are erythematous to violaceous annular plaques that last days to weeks and fade with a residual purpuric stain. Other features include hepatomegaly, peripheral lipodystrophy, arthralgia, nodular episcleritis, conjunctivitis, auricular and nasal chondritis, splenomegaly, anemia and aseptic meningitis.
Skin lesions show an extensive mixed dermal and subcutaneous inflammatory infiltrate composed predominantly of atypical myeloid cells and mature neutrophils in addition to eosinophils and mononuclear cells.
The 'pathological misfit' is the 'eyeliner' sign.
This sign seen in Bowen's disease refers to the intact normal basal layer despite the full thickness atypia of the rest of the epidermis.
The other mentioned signs are features of mycosis fungoides (MF). In early MF, atypical lymphocytes line up along the dermoepidermal junction demonstrating epidermotropism (row of toy soldiers or string of pearls appearance). Large atypical lymphocytes lying singly within the epidermis having irregular hyperchromatic nuclear contours with clear perinuclear haloes are likened to a 'lump of coal on a pillow'. A relatively unreliable sign encountered in some cases of MF is the 'bare underbelly sign' which describes the presence of lymphocytes on the epidermal side of the superficial vascular plexus, an indication of their epidermotropic nature.
Pigmented DFSP/Bednar tumor
Statement b is incorrect.
Bednar tumor is a variant of DFSP, very common in Africans or African-Americans. It is characterised by dermal-based spindle cells arrayed in a storiform and fascicular pattern. Dendritic melanocytes are interspersed. It is locally aggressive. Immunohistochemically, the neoplastic cells express CD34, which may be lost during transformation to higher grade malignancy. The melanocytes express S100. Factor XIIIa, which marks dermatofibromas is negative in this tumor.
The eponym is 'Masson'.
Claude L. Pierre Masson (12th November 1880 – 11th May 1959) was a French born histopathologist from Quebec. Despite having a keen interest in clinical medicine, he studied basic sciences and became one of the most famous pathologists of his time. His name was entered in the 'Canadian Medical Hall of Fame' in 1997.
The Masson's trichrome is a three color staining protocol used to distinguish various connective and soft tissue elements. Muscle fibres stain red and collagen green.
Masson's pseudoangiosarcoma ( hemangio-endotheliome vegetant intravasculaire or Masson's hemangioma or papillary endothelial hyperplasia) was described by Masson in 1923 as a neoplastic process mimicking angiosarcoma in infected hemorrhoidal veins. It is now known to be an unusual organization of a thrombus within a vein or within vessels of various vascular anomalies such as cavernous hemangiomas, lymphangiomas and pyogenic granulomas. Clinically, it presents as single or multiple, small, occasionally painful, firm blue nodules. Microscopically, it is a widely dilated vascular channel in the dermis or subcutis containing an organizing thrombus and blunted papillary projections with a hyalinized collagenous core. The papillae are lined by a single layer of plump endothelial cells that lack anaplasia or pleomorphism unlike angiosarcomas.
The Fontana- Masson stain is a silver stain that stains argentaffin granules and melanin black.
Corkscrew
The common descriptive terminology for all these conditions is "corkscrew".
The vascular pattern of melanoma on dermoscopy is termed as corkscrew. In syphilis, the spirochaetes have a corkscrew appearance on Warthin-Starry or other silver impregnation techniques. Fibromatoses comprises a group of proliferations spanning various age groups that may be locally aggressive and are characterised histologically by corkscrew-like myofibroblasts. In scurvy, one sees corkscrew hair and pinpoint haemorrhages around hair follicles. This feature is usually appreciated in adults.
Eccrine syringofibroadenoma
Eccrine syringofibroadenoma (ESFA) is an uncommon condition described by Mascaro in 1963. The age of onset ranges from 16 to 80 years, however, mostly it affects patients in their seventh and eighth decades. It may show a variable presentation, including solitary lesions, multiple papules and nodules arranged in a symmetrical or linear nevoid pattern, associated with hidrotic ectodermal dysplasia or as a reactive phenomenon occurring in inflammatory conditions like bullous pemphigoid, psoriasis, lichen planus, leprosy, etc.
Clinically, it presents as hyperkeratotic plaques usually on the extremities. Histopathology demonstrates thin anastomosing epithelial cords and strands forming a lattice and connected to the undersurface of the epidermis. The cells are smaller and more basophilic than the epidermal keratinocytes. Ducts are present within the tumor. Between the strands there is a rich fibrovascular stroma comprising of mast cells, lymphocytes and plasma cells. Carcinomatous transformation has been reported in long standing lesions.
Silver, causing argyria
Silver is used as a coating in many mouth fresheners including cardamom and betel nut, Jintan in Japan. Excess intake of silver imparts a slate-grey pigmentation.
Argyria is a rare cause of cutaneous discolouration caused by silver deposition. Argyria can be localized or generalized, depending upon the mode and amount of silver absorbed. In general, the macular pigmentation in argyria is slate-grey. It is more pronounced on sun exposed areas including face, neck, arms and dorsum of the hands. Mucosal/conjunctival involvement and azure lunulae (of nails) are characteristic attributes of argyria. Diagnostic histopathologic features are deposition of uniform fine brown black granules in the basal lamina of the secretory portion of eccrine glands, blood vessel walls and elastic fibres of the papillary dermis. To a lesser extent, deposits are also seen in the connective tissue sheath surrounding pilosebaceous units, perineural tissue and arrector pili muscles. Dark field microscopy under which the granules are brightly retractile is particularly useful in suspected cases of argyria where the deposits are not evident under light microscopy.
Eosinophil
Eosinophils are characterised by bright orange red granules and a bilobed nucleus. Eosinophilic dermal infiltrate is a feature of drug reactions and insect bites. In Well's syndrome, eosinophilic infiltrate forming flame figures is seen. Flame figures comprise of granules from eosinophils coating degenerate, blue collagen bundles in loci. Among bullous diseases, eosinophils are frequently encountered in bullous pemphigoid, pemphigus vulgaris and foliaceus.
Apocrine poroma
Poromas are skin adnexal neoplasms with prominent ductal differentiation, comprising of dark poroid and pale cuticular cells. The ducts are always seen within the cuticular cells. There are three architectural variants: hidroacanthoma simplex (confined to the epidermis and sharply demarcated), classic poroma (aggregates that protrude into the upper dermis) and dermal duct tumor (tumor cells situated deep within the reticular dermis). Poromas can be eccrine or apocrine. Eccrine poromas classically occur on the extremities. In contrast, apocrine poromas are common on the head and neck and show continuity with infundibular structures. It is important to note that necrosis and mitoses are common in poromas and do not indicate malignancy.
Dowling Degos Disease
The statement given in the question is a memorable description of Dowling–Degos disease by Wilson-Jones and Grice (see reference below).
Dowling–Degos disease is also known as reticulate pigmented anomaly of the flexures. It is an autosomal dominant disorder that affects the skin of the back, neck and axillae in the form of pigmented, reticulate macules/papules .There might be also pitted perioral or facial scars. Mutation in keratin 5 (KRT5) was found in this disorder. Galli–Galli disease is the acantholytic variant of this disease.
Histopathology shows elongated, pigmented rete ridges (filiform, “antler-like” downgrowths); thinning of suprapapillary epithelium; perivascular infiltrate and dermal melanosis.
Differential diagnoses include reticulate acropigmentation of Kitamura and adenoid form of seborrheic keratosis, although the downgrowths are more digitate than in seborrheic keratosis and there is no papillomatosis.
Reference:
Wilson-Jones E, Grice K. Reticulate pigmented anomaly of flexures (Dowling–Degos): a new genodermatosis? Br J Dermatol 1974; 91 (Suppl. 36): 6
CD 14. The rest are markers for mast cells.
Immunostains are of great help in diagnosing mast cell (MC) disorders.
Tryptase: positive in all mast cells, normal or neoplastic, granular, intracytoplasmic staining.
CD117: membranous staining, together with tryptase helps in differentiating mast cells from basophils.
CD2: weak positive in neoplastic mast cells, even stronger in surrounding reactive lymphocytes
CD25: positive in neoplastic mast cells.
Presence of mast cells which co-express CD117 and CD2 and/or CD25 is one of the minor criteria for the diagnosis of systemic mastocytosis.
CD 14 is a monocytic/histiocytic marker. Mast cells do not stain with it.
Fibrofolliculoma
The other three tumors i.e. cylidroma, spiradenoma and trichoepithelioma are components of Brooke-Spiegler syndrome, an autosomal dominant syndrome with mutations in the CYLD gene on chromosome 19q. Salivary gland tumors are also seen. Multiple Fibrofolliculomas and Trichodiscomas, on the other hand, are seen in Birt-Hogg-Dube syndrome, characterised by mutations in the BHD gene on 17p. These patients may also have renal tumors and lung cysts.
Hidradenitis suppurativa
All the other diseases show foamy histiocytes as a distinctive finding while hidradenitis suppurative does not.
Verruciform xanthoma. On the basis histological appearance the epithelial changes in verruciform xanthoma have been been divided into three groups-verrucous, papillary, and flat-and these epithelial changes reflect the clinical picture of the lesion. The diagnostic histological finding, however, whether intra- or extraoral in location, is the presence of foam cells that fill the dermal papillae and submucosal space. These foam cells have been shown to have monocyte/macrophage lineage.
CHILD syndrome. Histopathological examination reveals psoriasiform epidermal hyperplasia and, sometimes, verruciform xanthoma like features, i.e., foamy histiocytes in the upper papillary dermis.
Fox Fordyce disease. There is an associated mild to moderate inflammatory cell infiltrate which may contain some neutrophils as well as chronic inflammatory cells. Perifollicular foam cells have been found to be a relatively consistent and distinctive feature.
Hidradenitis suppurativa. In established lesions, there is a heavy, mixed inflammatory cell infiltrate in the lower half of the dermis, usually with extension into the subcutis. Chronic abscesses are present in active cases and these may connect with sinus tracts leading to the skin surface. The sinuses are usually lined by stratified squamous epithelium in their outer part. Granulation tissue containing inflammatory cells and occasional foreign body giant cells is present in up to 25% of cases. Inflammation of the apocrine glands may be present in the axillary region in about 20% of cases. Perieccrine inflammation is seen in approximately one-third of cases, from all sites. In early lesions, there is folliculitis and perifolliculitis involving the lower part of the follicle. The infundibulum is usually dilated and contains keratinous material and inflammatory debris. These findings support the notion that acne inversa is primarily a follicular disease, but apocrine glands can be primarily involved in a minority of axillary lesions.
The term Gorlin links all of these.
The nevoid basal cell carcinoma syndrome, also known as Gorlin’s syndrome, is a multisystem disorder characterized by multiple basal cell carcinomas with an early age of onset, odontogenic keratocysts, pits on the palms and/or soles, cutaneous cysts, skeletal and neurological anomalies, and ectopic calcifications. Often there is a characteristic facies, with hypertelorism and an enlarged skull. Less common manifestations include lipomas and fibromas of various organs, fetal rhabdomyoma, unilateral renal agenesis, adenoid cystic carcinoma of minor salivary gland, ovarian cysts, and medulloblastomas. Its prevalence is estimated to be 1 in 57 000 to 1 in 164 000. The inheritance is autosomal dominant with mutation in the patched homologue 1 (PTCH1) gene on chromosome 3.
Goltz-Gorlin syndrome is the other name for focal dermal hypoplasia, in which the skin biopsy shows reduced thickness of the dermis, with some thin, loosely arranged collagen fibers in the papillary dermis. Clusters of adipocytes may be anywhere in the dermis or in a perivascular location. The extreme degree of attenuation of the collagen seen in focal dermal hypoplasia is not present in nevus lipomatosus, in which mature fat also replaces part of the dermis; furthermore, the clinical presentations of the two conditions are quite distinct.
Gorlin sign is the ability to touch the tip of the nose with the tongue. It is seen in 50% of patients of Ehlers-Danlos syndrome.
Erythema toxicum neonatorum
It is characterised by eosinophilic infiltrates in biopsy from a pustule while all the rest are predominantly neutrophilic.
All these entities are differential diagnoses for vesiculopustular lesions in a neonate. Erythema toxicum neonatorum is a common, self-limited entity which appears within the first few days of life as erythematous macules, papules, and pustules, mostly located on the trunk. The lesions resolve within a few days leaving no sequelae. There are subcorneal or intraepidermal pustules, filled with eosinophils and related to the orifices of the pilosebaceous follicles. An inflammatory infiltrate composed predominantly of eosinophils is present in the upper dermis in the vicinity of the follicles, and there is some exocytosis of these cells into the epithelium of the involved follicles.
Transient neonatal pustular melanosis is an uncommon condition that presents at birth with pigmented macules, often with a distinct collarette of scale, and vesiculopustules which are clustered beneath the chin, on the forehead, the neck and the back, and sometimes on the extremities. The vesiculopustules usually resolve after several days, often transforming into pigmented macules. The pigmented lesions persist for several weeks or more and then slowly fade. The vesiculopustules are intracorneal or subcorneal collections of neutrophils, admixed with fibrin and a few eosinophils. There may be a mild infiltrate of inflammatory cells around vessels in the upper dermis.
Acropustulosis of infancy is an uncommon pustular dermatosis characterized by recurrent crops of intensely pruritic vesiculopustules on the distal parts of the extremities of infants. The lesions measure 1–2 mm in diameter. Its onset is at birth or in the first few months of life, and resolution occurs at 2–3 years of age. There is an intraepidermal pustule containing neutrophils and sometimes varying numbers of eosinophils. This progresses to form a subcorneal pustule.
Miliaria pustulosa is characterized by neutrophils beneath the stratum corneum and/or in the epidermal sweat duct.
Neonatal acne or benign cephalic pustulosis is characterised by inflamed papules and pustules on the face of neonates. Skin biopsy from these shows follicular pustules with neutrophils.
Jadassohn
Borst-Jadassohn phenomenon is characterised by well-demarcated nests of uniform, basaloid cells confined within the epidermis, most often associated with benign lesions such as seborrheic keratosis (especially if irritated by infection or trauma) or entirely intraepidermal sweat gland tumors (hidroacanthoma simplex of Smith and Coburn). Less commonly, it may be seen in clonal actinic keratosis, Bowen's disease, melanoma in situ, Paget's disease and epidermotropic metastatic carcinomas.
Jadassohn-Lewandowski Syndrome is the other name for pachyonychia congenital, an autosomal dominant disorder with mutation in the highly conserved 1A domain of K6, K16 and K17 (chromosome 17). The characteristic features include:abnormally thick curved nails (onychogryposis)/ wedged door abnormality, palmoplantar keratoderma, palmoplantar hyperhidrosis and oral leukoplakia.
Common blue nevus is also known as Jadassohn-Tie`che blue nevus as it was first described by Tie`che, a student of Jadassohn in 1906. Common blue nevus is a grey-black macule or a papule commonly found on dorsae of extremities and head and neck regions. Other variants of blue nevus are cellular, combined, sclerosing and epithelioid blue nevi. Histopathologically, there are elongated dendritic melanocytes in the interstices of collagen in upper and mid dermis in common blue nevus. Cellular blue nevus additionally shows some islands of epithelioid cells and plump spindle cells, with abundant cytoplasm. Dermal fibrosis is a prominent finding along with dendritic melanocytes in the dermis in sclerosing blue nevus. Combined blue nevus shows a junctional melanocytic nevus along with the features of common blue nevus.
Naegeli-Franceschetti-Jadassohn Syndrome (MIM 161000) is a rare autosomal dominant form of ectodermal dysplasia that results from mutations in the KRT14 gene located on chromosome 17q11.2-q21. It is characterised by complete absence of the patterned ridges on the skin of the hands and feet, called dermatoglyphics that are the basis for each person's unique fingerprints, reticulate pattern of skin hyperpigmentation, palmoplantar keratoderma, abnormal sweating and enamel defects. It closely resembles dermatopathia pigmentosa reticularis and is distinguished by lifelong persistence of the skin hyperpigmentation, partial alopecia, and absence of dental anomalies in dermatopathia reticularis pigmentosa.
Calcaneal petechiae/talon noir, Benzidine stain
This condition, also known as black heel, presents with dark spots of recent origin usually on the soles of the feet. Lesions are usually bilateral and there is a history of jogging or prolonged walking, hence it affects young people or athletes more often. Eruptive nevi, lentigenes, acral nevi/melanoma may be considered as the differential diagnoses, especially when it is not suspected clinically.
Skin biopsy shows findings confined to the stratum corneum which shows intracorneal hemorrhage. Depending on how old the hemorrhage is, there can be RBCs, or an orange-yellow stained crust. This material stains negatively with Perls stain for hemosiderin but often stains positive with benzidine for hemoglobin.
Dermoscopy has also been used for diagnosis. It shows homogenous reddish pigmented globules of hemorrhage. Sometimes this may be arranged along the crests giving a parallel appearance, mimicking acral melanoma.
It has been suggested that paring alone may reveal blood in the stratum corneum obviating the need for a biopsy. Once the pigmentation is confirmed to be due to blood, the diagnosis is established and other conditions can be safely excluded. Lesions resolve spontaneously in a few days, but may recur.
Onion skin pattern
Borderline leprosy: perineural onion skin fibrosis.
Erythema elevatum diutinum: perivascular onion skin fibrosis in late lesions.
Lipoid proteinosis: perivascular onion skin hyaline deposits.
Perineuroma: sclerosing perineuroma shows a whorled onion skin growth pattern.
Myopericytoma: myoid cells/pericytes arranged concentrically in onion skin pattern around blood vessels.
Beaded
Elastofibroma shows beaded coarse elastic fibres. Trichorhrexis nodosa shows beaded hair shaft. The granule of actinomycetoma is composed of beaded gram positive filaments. Beaded eyleid papules are a characteristic clinical finding in lipoid proteinosis, Atypical mycobacteria especially Mycobacteria kansasii shows a coarsely beaded appearance on acid fast staining.
Mycosis fungoides
Mycosis fungoides does not show the presence of a grenz zone. A grenz zone can be seen in 48% cases of nodular PKDL, 75% cases of erythema elevatum diutinum and 70% cases of dermatofibroma. It is important to note that the presence of grenz zone, earlier considered to differentiate granuloma faciale from erythema elevatum diutinum is no longer used to differentiate between these two entities.
The term Gottron links all of these.
Progressive symmetric erythrokeratoderma,also known as Gottron's syndrome, is characterized by well-defined, erythematous, hyperkeratotic plaques distributed mainly on the knees, elbows, buttocks, head and dorsal surfaces of the hands and feet. Onset is during early childhood. The histopathological findings are not distinctive. There is hyperkeratosis, irregular acanthosis, very mild papillomatosis in some biopsies, and a mild superficial perivascular infiltrate of lymphocytes. Dyskeratotic, grainlike cells may be seen in the lower stratum corneum. There may be parakeratosis and some vacuolation in the lower horny cells and in the granular layer.
Papillomatosis cutis carcinoides, also known as Gottron tumor, consists of a group of verrucous carcinomas that are locally invasive and destructive but rarely metastasize.
Acrogeria is also called Gottron’s syndrome. It is an exceedingly rare disease, with onset in early childhood. There is atrophy, dryness, and wrinkling of the skin which is most severe on the face and extremities. Associations include bony abnormalities and disorders of dermal elastic tissue in the form of elastosis perforans serpiginosa and perforating elastomas. There is atrophy of the dermis with degenerative changes in the collagen. Fibers may be swollen and present a ‘boiled’ appearance. The subcutaneous fat is often replaced by connective tissue which is indistinguishable from the dermal collagen. Elastic fibers are disrupted and irregular, with some clumping.
Tumor of follicular infundibulum
This is an uncommon benign adnexal tumor that usually presents as a solitary keratotic papule in the head and neck area in elderly. Infrequently, it may present as multiple lesions or in association with syndromes like the Schöpf–Schultz–Passarge syndrome and Cowden’s syndrome.
Histopathologically, the tumor is comprised of a superficial horizontal plate-like proliferation of eosinophilic, pale-staining keratinocytes with a peripheral palisading of basaloid cells. Mutifocal connections between tumor strands, epidermal surface and existing follicular structures can be seen, creating a reticulated pattern. Some cases also contained small horn microcysts with keratohyaline granules and small tubular structures with an eosinophilic wavy lining resembling sebaceous ducts. Occasionally, the infundibulocystic structures appeared to be connected to entrapped follicles in the lesions. It shows a characteristic staining pattern, with abundant glycogen highlighted by periodic acidSchiff (PAS) staining, and prominent elastic fiber ‘sheathing’ around the tumor collections. The brush-like elastic network helps distinguish tumor of follicular infundibulum from basal cell carcinoma and seborrheic keratoses, which lack this feature.
Clear cell papulosis
This is an extremely rare entity affecting children in the age group of 1-4 years. It is considered to be a benign counterpart of extra-mammary Paget’s disease. Affected patients present with hypopigmented macules and papules on the anterior chest and abdomen, usually along the milk line. These resolve spontaneously with age.
Biopsy from involved skin shows acanthosis and ‘clear cells’ which are large keratinocytes mainly found in the basal layer of epidermis and in lesser numbers in the upper layers. These cells contain abundant mucin. Focal clustering and nuclear grooving of these cells has been observed by some authors. The cells closely resemble Toker cells in the nipple as well as Paget cells but can be differentiated by the presence of intra-cytoplasmic mucin in clear cell papulosis, which is not seen in Toker cells. The immunohistochemical profile of these cells suggests an eccrine origin as they stain with carcinoembryonic antigen, cytokeratin CK-7, epithelial membrane antigen and IKH-4 antibody and do not stain or stain weakly with gross cystic disease fluid protein antigen.
Paget cells, on the other hand, stain strongly with gross cystic disease fluid protein antigen, suggesting an apocrine origin. The clinical features, age of onset and immunohistochemistry are helpful in differentiating clear cell papulosis from other conditions with clear cells in the epidermis including extra-mammary Paget’s disease, pagetoid squamous cell carcinoma, sebaceous carcinoma and pagetoid melanoma.
The hypopigmentation may be due to a defect in melanogenesis as suggested by a report of reduced melanin pigment in the areas of epidermis occupied by clear cells.
In clear cell/pale cell acanthoma, solitary or multiple brownish nodules are present on the legs of middle aged individuals that show large pale staining keratinocytes in acanthotic epidermis.
Paisley-tie pattern
Paisley tie tumors are a histological group of tumors consisting of syringomas as prototype along with desmoplastic trichoepithelioma, morpheic basal cell carcinoma and microcystic adnexal carcinoma.
Syringomas are dermal tumors composed of multiple small ducts lined by two layers of cuboidal epithelium.
Desmoplastic trichoepitheliomas are composed of cords and small nests of basaloid cells with scanty cytoplasm. Tumor strands may be attached to the epidermis. There are usually many keratinous cysts, with a peripheral basaloid layer and several layers of stratified squamous epithelium with central loosely laminated horn. Comma shaped epithelial projections extend from the peripheral layer of some of the keratinous cysts. The tumor cells do not contain carcinoembryonic antigen, unlike the cells in a syringoma, which are usually positive. In contrast, involucrin is expressed in desmoplastic trichoepitheliomas but not in syringomas. Merkel cells (CK20) are present in desmoplastic trichoepitheliomas but are uncommon in basal cell carcinoma.
Microcystic adnexal carcinoma usually involves the subcutis as well as the dermis, and it may extend into the underlying muscle. The superficial part is composed of numerous keratinous cysts and small islands and strands of basaloid and squamous epithelium showing variable ductal differentiation. Perineural invasion is frequently present. The aggressive growth and perineural spread allow a distinction to be made from syringoma and desmoplastic trichoepithelioma. In some of the reported cases of microcystic adnexal carcinoma, the luminal cells were CEA positive.
Sclerosing or morpheic type of basal cell carcinoma shows narrow elongated strands and small islands of tumor cells embedded in a dense fibrous stroma. Ber-EP4 is positive focally in most trichoepitheliomas, contrasting with the usual diffuse staining in basal cell carcinoma.
Lipoid proteinosis
Lipoid proteinosis, also known as hyalinosis cutis et mucosae, is a rare autosomally recessive disorder characterized by widespread deposition of hyaline material in the skin, mucosa, and various internal organs. It was first described in 1929 by two Viennese, E. Urbach and C. Wiethe, a dermatologist and an otorhinolaryngologist, as lipoidosis cutis et mucosae based on the deposition of lipoid material with protein in the skin and mucous membranes. It was renamed as lipoid proteinosis to avoid confusion with other lipidoses. The first clinical presentation of lipoid proteinosis is usually hoarseness of voice due to infiltration of the laryngeal mucosa, which usually appears in early childhood. Cutaneous lesions develop afterwards or simultaneously. Skin lesions occur in two phases. Vesiculo-bullous lesions, pustules, and hemorrhagic crusting of the skin and mucosae characterize the first stage (inflammatory). These lesions heal with “ice pick” acneiform scarring, mainly over the face and distal extremities. In the second phase, yellowish waxy papules, nodules, and plaques occur over the face. Hyperkeratotic verrucous plaques may also be seen around the elbows or knees. Rarely, generalized infiltration may develop. Beaded papules over the palpebral margin of the eyelid, known as ‘moniliform blepharosis’ are characteristic of lipoid proteinosis. The mucosae of the pharynx, vocal cords, tongue and lips show an infiltration similar to that seen in the skin. The tongue is firm and enlarged with restricted mobility. Lesions may also be present in the soft palate, uvula, epiglottis, aryepiglottic fold, and, rarely, in the mucosa of the labia and vagina. Other uncommon manifestations include dental anomalies like hypoplasia or aplasia of teeth, patchy alopecia, diffuse hair loss, and recurrent parotitis. Widespread visceral involvement has been described, although few cases develop significant clinical symptoms. Neurologic manifestations are common and include psychomotor and grand mal seizures, memory loss, and schizophrenia. The pathognomonic finding in the CT scan of the head is bilateral, intracranial, sickle shaped calcification within the temporal lobe of the brain.
Histological examination of the lesional skin with hematoxylin-eosin stain shows progressive deposition of pale, eosinophilic, hyaline material in the superficial dermis, but this is initially localized around small blood vessels and at the periphery of eccrine sweat glands. In advanced lesions, the deposits around blood vessels may have an ‘onion-skin’ appearance. The epidermis may show hyperkeratosis and some acanthosis in the verrucous lesions. The hyaline deposits are PAS positive and diastase resistant. They stain positively with colloidal iron and Alcian blue at pH 2.5 and also with Sudan black and oil red O on frozen sections. Ultrastructurally, fine collagen fibrils, embedded in an amorphous matrix, are seen. There is prominent reduplication of the basal lamina at the dermoepidermal junction and concentrically around vessels.
Porphyria also shows similar amorphous deposits in skin biopsy. However, the deposits in the latter condition are more limited in distribution, being perivascular only. Sweat glands are not involved in porphyria.
Miescher’s radial granuloma
Erythema nodosum is the prototype septal panniculitis without vasculitis. The septa of subcutaneous fat are thickened and infiltrated by inflammatory cells that may extend to the periseptal areas of the fat lobules. The composition of inflammatory infiltrate in the septa varies with age of the lesion. In early lesions, edema, hemorrhage, and neutrophils are seen whereas fibrosis, periseptal granulation tissue, lymphocytes, histiocytes and multinucleated giant cells are the main findings in late stage lesions. A histopathologic hallmark of erythema nodosum is the presence of Miescher’s radial granulomas, that consist of small, well-defined nodular aggregations of small histiocytes around a central stellate or banana shaped cleft. In older nodules of erythema nodosum, histiocytes coalesce to form multinucleated giant cells, many of which still retain in their cytoplasm a stellate central cleft reminiscent of those centers of Miescher’s radial granuloma. Sometimes, Miescher’s radial granulomas are conspicuous in the septa, but occasionally serial sections may be necessary to identify them. Recent immunohistochemical studies have demonstrated that the central cleft of Miescher’s radial granulomas express myeloperoxidase, which suggest that myeloid cells were present in some stage of formation.
A close differential diagnosis is subcutaneous histiocytoid Sweet's syndrome that can show Miescher's radial granulomas as well as histiocytic giant cells and clusters of mononuclear small oval cells that stain positively with myeloperoxidase. Due to these similar findings it is hypothesised that erythema nodosum and histiocytoid Sweet's syndrome may be linked.
Cornoid lamellation
Cornoid lamellation is a reaction pattern which was first described by Mibelli in 1893 and is characterised by the presence of a narrow parakeratotic column. Cornoid lamella is thought to be formed by a genetically determined mutant clone of atypical epidermal keratinocytes. Porokeratosis is the prototype disorder in which this pattern is seen. Lamellar bodies, which contain lipid substances that function as a permeability barrier of the horny layer, also have acid hydrolase which causes desquamation of horny cells. Stacking of cornoid lamella horny cells may result from decreased number of lamellar bodies which brings about a defect of desquamation.
Cornoid lamellation is a change that is confined to the edge of clinical lesions and it is essential that the margin of the papule or plaque be biopsied. Some have recommended the use of gentian violet to highlight the keratotic borders, though this is not usually required.
Cornoid lamellation is characterized by a thin column of parakeratotic cells that extends through the surrounding orthokeratotic stratum corneum and to some extent above and below it. There is a marked decrease in or loss of the granular zone beneath the column of parakeratosis. Of considerable diagnostic significance is the presence of dyskeratosis or vacuolization of cells in the underlying spinous layer, just beyond the lower end of the parakeratotic column and serves to distingish the cornoid lamella from other ordinary columns of parakeratosis.The parakeratotic column is often oriented slightly obliquely with its tip slanting inwards. The papillary dermis beneath the column shows dilated capillaries with a moderately dense lymphocytic infiltrate. Multiple enlarged cornoid lamellae have been described in linear porokeratosis and in penoscrotal porokeratosis. The changes of cornoid lamellation restricted to the hair follicle have been reported.
Ultrastructurally, there is a decrease in keratohyaline granules and lamellar bodies underneath the cornoid lamella. Dyskeratotic cells beneath the cornoid lamella have vacuolated cytoplasm. Some of these vacuoles were noted to be due to vacuolated mitochondria. The cells in the parakeratotic column were flattened, more compact and had electron dense cytoplasm. The homogenous eosinophilic appearance of cornoid lamella seems to be due to stacking of ultrastructurally compact horny cells.
Porokeratosis is the prototype disorder in which cornoid lamella is observed. Wade and Ackerman observed that cornoid lamellation occurred in conditions other than porokeratosis such as seborrheic keratoses, verruca vulgaris, scar, milia, solar keratosis, squamous cell carcinoma in situ and basal cell carcinoma. It can also be seen in inflammatory disorders such as psoriasis, lichen planus like keratosis, dermatomyositis, keratosis lichenoides chronica, Grover's disease and Fox Fordyce disease.
Argyria
There is a wide individual variation in the quantum and duration of exposure required to produce argyria. Following systemic intake, argyria results in an ashy to blue-black, diffuse pigmentation that affects both the skin and mucosae. The slate blue colour is due to both silver salts as well as increased melanin.
Biopsies from argyric skin appear normal at first glance apart from some increase in epidermal melanin content. On higher magnification, there are several, distinctive, uniformly sized, tiny black dots in vessel walls, around eccrine glands and in the connective tissue sheaths around hair follicles. In addition, smaller numbers may be seen lying free in the dermis.
Cutaneous silver deposits are also detectable using dark ground microscopy and electron microscopy, which may be useful in cases where no findings are seen in light microscopy. The appearance of silver deposits in dark ground microscopy is also known as ‘stars in heaven’ pattern. Electron dense deposits measuring around 100-500 nm are seen in electron microscopy.
Prurigo pigmentosa
All except prurigo pigmentosa show superficial and deep perivascular mononuclear and lymphoid infiltrates. The differential diagnosis of this pattern can be remembered by the mnemonic 8Ls+ Drugs and include:
Eight ‘L’s
Light reactions,
Lymphoma (including pseudolymphomas),
Leprosy,
Lues (syphilis),
Lichen striatus,
Lupus erythematosus,
Lipoidica (includes necrobiosis lipoidica),
Lepidoptera (insect bite hypersensitivity, parasites).
+ ‘DRUGS’
Prurigo pigmentosa shows a predominantly superficial infiltrate. In the initial phase there is a superficial perivascular and interstitial infiltrate of neutrophils. This is followed by neutrophilic spongiosis and focal epidermal microabscesses, accompanied by ballooning and degeneration of keratinocytes. This is followed by the influx of eosinophils and lymphocytes into the upper dermis. The epidermis becomes variably hyperplastic, parakeratotic, and hyperpigmented. In later stages there is prominent melanin incontinence with numerous melanophages in the dermis.
Necrotizing infundibular crystalline folliculitis
Necrotizing infundibular crystalline folliculitis (NICF) is a rare cutaneous disorder with multiple waxy folliculocentric papules appearing on seborrheic areas, particularly forehead, neck and back in adults.
The term was first used in 2001 by Kossard and colleagues. NICF is both a distinct entity and an epiphenomenon in the vicinity of epithelial skin neoplasms (secondary NICF). Histology shows follicular invagination containing filamentous birefringent crystalline deposits, enclosed by parakeratotic columns, with an underlying, partly necrotic, follicular epithelium. The filamentous material contains birefringent urate-like crystals, which are represented as Alcian blue-positive mucinous material. Perifollicular neutrophils have been observed in a few cases. On electron microscopy, the crystalline material is composed of disrupted bundles of tonofilaments embedded in an amorphous matrix.
The etiology of this entity is not yet well understood. It remains unclear whether the presence of Malassezia or Propionibacterium in the infundibulum of follicles plays a crucial role in the induction of crystalline structures or mucin. Sebum accumulation as a nutrient medium for the microorganisms has been discussed, accompanied by the accumulation of crystalline material due to the destruction of tonofilaments and the degradation of lipids, followed by a rupture of follicular epithelium and accumulation of inflammatory cells.
Clinical response to topical or systemic antibiotic and antimycotic therapies supports the theory of microbial involvement in NICF. Another possible mechanism inducing the crystalline material seems to be a chemical or physical injury. Recently NICF has also been reported to be induced by targeted anti-tumor therapies like EGFR and VEGF inhibitors.
Basal cell carcinoma
Immunohistochemical staining for cytokeratin 20 (CK20) is positive in fibroepithelioma of Pinkus, Merkel cell carcinoma, trichoepithelioma and secondary forms of extra-mammary Paget’s disease but not in basal cell carcinoma. CK20 is a marker of Merkel cells, and has been used to differentiate certain forms of trichoepitheliomas (desmoplastic) and fibroepithelioma of Pinkus from BCC, which rarely expresses CK20.
Trichoepithelioma and BCC are seen as basaloid nests in dermis. A connection with overlying epidermis is seen in one-third of trichoepitheliomas. Abortive hair follicles and keratinous cysts are additional features seen in trichoepitheliomas.
Fibroepitheliomas show anastomosing cords of basaloid cells arising from epidermis with a fibrovascular stroma and with prominent Merkel cells (seen in 85% of cases). The origin of fibroepithelioma is controversial. It has been considered as a variant of basal cell carcinoma as well as trichoblastoma. The malignant potential is also uncertain.
Paget’s disease shows cells with abundant pale cytoplasm and large nuclei in epidermis, rarely extending to dermis. Extra-mammary Paget’s disease (EMPD) additionally shows abundant mucin. Cells in Paget’s disease show positive immunostaining for CEA, CA15.3, CD5 and 23, low molecular weight cytokeratins, epithelial membrane antigen and gross cystic disease fluid protein (GCDFP) variably. Cytokeratin immunophenotype has been used to distinguish primary and secondary forms of EMPD, with CK7+/CK20- seen in former and CK7-/CK20+ seen in latter.
Merkel cell carcinoma shows small cells with scant cytoplasm, arranged in trabeculae, solid nests or infiltrating sheets in dermis. CK20 is characteristically expressed with paranuclear dot-like staining.
Human Polyomavirus 7 associated pruritic rash and viremia in transplant recipients
Till now only 2 polyoma viruses were known to cause skin disease in humans, these are Merkel cell polyomavirus and Trichodysplasia spinulosa polyoma virus. HPyV7 virus has been recently discovered by gene amplification studies to cause a distinctive pruritic rash in transplant recipients, appearing as velvety plaques specially on trunk. Histopathological changes are also distinctive, showing viral inclusion bodies in keratinocytes, resembling peacock plumage.
Reference: Ho J, Jedrych JJ, Feng H et al. Human Polyomavirus 7- associated pruritic rash and viremia in transplant recipients. J Infect Dis 2015:211;1560-5.
Granuloma faciale
Granuloma faciale usually presents as a solitary well-demarcated erythematous facial plaque or nodule with prominent follicular openings and telangiectasias. Multiple lesions are seen in one-third of cases. It is a misnomer as ‘granuloma’ suggests a histological finding of granulomatous inflammation, which does not occur. Early lesions show changes like leukocytoclastic vasculitis. The distinctive changes develop with time. In addition to dense infiltrates of neutrophils, eosinophils and plasma cells, fibrosis supervenes, often oriented concentrically around small vessels. A grenz zone separates the infiltrate from overlying epidermis. Eosinophilic angiocentric fibrosis is a rare fibrosing condition that shares many histologic characteristics with GF and is regarded by some authors as a mucosal counterpart of granuloma faciale. Cases of granuloma faciale with concurrent eosinophilic angiocentric fibrosis in larynx have been reported.
Erythema elevatum diutinum
Granuloma faciale, Kimura’s disease and Rosai-Dorfman disease show IgG4 positive plasma cells in skin biopsy, while erythema elevatum diutinum shows IgG4-negative plasma cells.
IgG4 related disease is a polymorphic group of inflammatory pseudotumors formed by IgG4 specific plasma cells. Granuloma faciale shows significant overlap and can be difficult to dintinguish from IgG4 related disease. Kimura’s disease shows overlapping features of inflammatory nodules with IgG4 positive plasma cells, but is distinct from this group. Tissue and peripheral eosinophilia, reactive vascular proliferation, expression of IgE in follicular dendritic cells and eosinophilic microabscesses are features of Kimura’s disease, and not IgG4 related disease. Rosai-Dorfman disease shows IgG4 positive plasma cells. However it is unrelated to IgG4 related diseases. S100 positive histiocytes are seen in the former only.
Diagnostic criteria for IgG4 related disease are: 1) clinical examination shows characteristic diffuse/ localized swelling/ masses in single or multiple organs, 2) haematological examination shows elevated serum IgG4 (135 mg/dL), 3) histopathologically, there is a) marked lymphocyte and plasma cell infiltration and fibrosis, and b) IgG4/IgG positive cells>40% and >10 igG4 positive plasma cells/ high power field. All 3 criteria are needed for definite diagnosis, 1 and 3 for probable diagnosis and 1 and 2 for possible diagnosis. Eosinophilic infiltrates are described in all these disorders. Leucocytoclastic vasculitis can be seen in granuloma faciale and erythema elevatum diutinum.
Halogenoderma
Halogenoderma is characterized by eruption of papules, pustules and crateriform exudative plaques in a generalised distribution. Skin biopsy shows pseudoepitheliomatous hyperplasia with neutrophilic microabscesses, raising suspicion of keratoacanthoma and infection. Pus cultures are negative. It is caused by hypersensitivity to iodides and bromides, found in certain bromine containing drugs such as iptratropium bromide. Excessive consumption of a soft drink containing brominated vegetable oil was reported to be the cause in some patients. Although brominated vegetable oil is now banned from cola beverages, it is still a component of diet coke (a favourite drink of US presidents!). Hence taking this history is crucial as discontinuation leads to spontaneous resolution.
Source: James WD, Berger TG, Elston DM (eds). Contact dermatitis and drug reactions. Andrews' Diseases of the Skin: Clinical Dermatology. Saunders. 2016;132-3.
Netherton’s syndrome
It is a rare autosomal recessive disease characterized by the triad of ichthyosis, trichorrhexis invaginata (bamboo hair), and an atopic diathesis with elevated levels of IgE. Affected neonates are born with ichthyosiform erythroderma, which becomes milder with age and develop into polycyclic ichthyosis or ichthyosis linearis circumflexa. There is a characteristic hair shaft anomaly i.e. trichorrhexis invaginata (bamboo hair) where cup-like expansion of the proximal part of the hair shaft surrounds the club-shaped distal segment in the manner of a ball-and-socket joint. Because of atopic diathesis hay fever and asthma are common in affected individuals.
Eosinophilic pustular folliculitis
Eosinophilic pustular folliculitis is a heterogeneous group of disorders, consisting of the classic form, eosinophilic pustular folliculitis or Ofuji's disease, HIV-associated eosinophilic pustular folliculitis and pediatric eosinophilic pustular folliculitis.
The classic form, eosinophilic pustular folliculitis or Ofuji's disease, is a rare, chronic dermatosis, first described in the Japanese. It is characterised by recurrent, sterile, follicular papules and pustules with a tendency to form circinate plaques. These may show central clearing with residual hyperpigmentation. Seborrheic areas, such as the face, trunk, and extensor surface of the proximal part of the limbs, are usually involved, but in 20% of cases the non-hair-bearing palms and soles may also be involved.
HIV-associated eosinophilic pustular folliculitis has been regarded as a subset of the pruritic papular eruption of HIV infection. It differs from the classic form by severe pruritus, the absence of circinate and palmoplantar lesions, and the less frequent involvement of the face.
Pediatric eosinophilic pustular folliculitis is usually confined to the scalp, although grouped aggregates of follicular pustules can occur on the face, extremities, and trunk in some patients. It usually has a self-limited course. The inclusion of this disorder in the group of eosinophilic pustular folliculitis has been debated because interfollicular inflammation is sometimes the predominant feature.
Histopathologically, there is eosinophilic spongiosis and pustulosis involving the infundibular region of the hair follicle. The infiltrate often extends into the attached sebaceous duct and sebaceous gland. Most follicles are preserved, but some show disruption or destruction of the wall by the inflammatory infiltrate. There is also a moderately dense, perivascular and perifollicular inflammatory cell infiltrate composed of lymphocytes, eosinophils, mast cells, and macrophages.
Granular parakeratosis
Granular parakeratosis is a unique epidermal reaction pattern reflecting an acquired disorder of keratinization, which may occur as a contact reaction to an antiperspirant, diaper or due to some unknown trigger. It is often restricted to intertriginous areas. Studies on granular parakeratosis have suggested a basic defect in the processing of profilaggrin to filaggrin which results in failure to degrade keratohyalin granules and to aggregate keratin filaments during cornification. Filaggrin mutations are known to be involved in the pathogenesis of ichthyosis vulgaris and atopic disorders.
Histopathologically, granular parakeratosis shows thickened stratum corneum with retention of keratohyalin granules. These granules are not seen beyond stratum granulosum in normal epidermis. Granular parakeratosis has been observed as an incidental finding overlying molluscum contagiosum, dermatomyositis, dermatophyte infection, and cutaneous carcinomas.
Nekam’s disease/ keratosis lichenoides chronica
Keratosis lichenoides chronica is a rare disease. It has often been a subject of controversy. It was first described as ‘lichen ruber moniliformis’ by Moritz Kaposi, a Hungarian dermatologist. Subsequently, it has been described as lichen ruber acuminatus, lichen ruber planus, porokeratosis striata lichenoides, and lichenoid trikeratosis. It is characterized by violaceous, papular, and nodular lesions in a linear and reticulate pattern on the extremities and a seborrheic dermatitis-like facial eruption. A rare vascular variant with telangiectasias has been reported. Oral ulceration and nail involvement may occur.
Keratosis lichenoides chronica may be associated with internal diseases such as glomerulonephritis, hypothyroidism, and lymphoproliferative disorders. Histopathologically, there is a lichenoid reaction pattern with prominent basal cell death and focal basal vacuolar change. The inflammatory infiltrate usually includes plasma cells, and there is deeper perivascular and periappendageal cuffing. Telangiectasia of superficial dermal vessels is sometimes noted. Epidermal changes are variable, with alternating areas of atrophy and acanthosis sometimes present, as well as focal parakeratosis.
Nevus sebaceous
The unifying feature in the three disorders, except nevus sebaceous, is the alternating pattern of epidermal findings. Actinic keratosis shows alternating pattern of parakeratosis due to sparing of follicular structures. Linear EHK and ILVEN show an alternating pattern of the underlying disease. This alternating pattern of underlying disease has also been found in blaschkoid VEN, linear psoriasis, and hyperpigmentary blaschkoid disorders.
Reference: Gupta V, Khandpur S, Arava S, Ramam M. Alternating histopathologic pattern in blaschkoid dermatoses with epidermal changes: A retrospective series of 61 cases. J Am Acad Dermatol 2018;78:812-3. .
Another histopathological feature that separates the other three entities from nevus sebaceous is epidermolytic hyperkeratosis. Epidermolytic hyperkeratosis is a histopathologic pattern that is seen in many conditions including linear EHK, ichthyosis bullosa of Siemens, epidermolytic keratoderma, epidermolytic acanthoma, and epidermolytic leukoplakia. It may also represent an incidental finding in ILVEN, seborrheic keratosis, actinic keratosis, in situ squamous cell carcinoma, invasive squamous cell carcinoma, melanocytic nevi, and epidermal and pilar cysts.
References:
Metze D. Disorders of keratinization. In: Calonje E, Granter SR, Mckee PH (eds). Mckee’s Pathology of the skin. 4th ed, Elsevier Saunders 2005: 1146–96.
Meibodi NT, Nahidi Y, Javidi Z. Epidermolytic hyperkeratosis in inflammatory linear verrucous epidermal nevus. Indian J Dermatol 2011; 56: 309–12.
Granuloma multiforme
Granuloma multiforme was first distinguished from tuberculoid leprosy by Leiker et al. It is also known as Unono enyl (=elephant ringworms) in Africa. The sun exposed sites of upper trunk and arms are mainly involved. Lesions begin as papules with pruritus and irritation and evolve into annular plaques with central clearing. Histology shows foci of necrobiosis surrounded by a granulomatous zone with elastotic material within the granulomas. Unlike granuloma annulare, granuloma multiforme shows dense perivascular infiltrates and absence of mucin, and absent palisading of cells. Annular elastolytic giant cell granuloma closely resembles granuloma multiforme. It is also known as actinic granuloma/ O’Brien’s granuloma. Unlike granuloma multiforme, actinic granuloma has many multinucleated giant cells and lacks necrobiosis.
Sclerosing lipogranuloma (paraffinoma)
Sclerosing lipogranuloma (paraffinoma) is a specific type of factitial panniculitis. Clinically, it presents as a painful rubbery indurated lesion, resulting from the injection paraffin into subcutaneous tissue (master’s zeal). Histopathologically, it is characterized by swiss-cheese appearance. There is disruption of fat cells and their replacement by cystic spaces of variable size, some surrounded by attenuated foreign body giant cells containing lipid vacuoles. There are bands of hyaline fibrous tissue between the fat cysts. The septa contain a scattering of lymphocytes and lipid-containing macrophages and foreign body giant cells.
Reticulate acropigmentation of Kitamura
Reticulate acropigmentation of Kitamura was first described in Japan in 1943 by Kitamura and Akamatsu. This occurs due to mutations in gene ADAM10 that results in aberrant Notch signalling pathway, which in turn affects keratinocyte and melanocyte proliferation. Clinically patients present with atrophic hyperpigmented macules with angulated borders that darken with time. Other features include palmar pits and break in dermatoglyphics (so escape a crime). Histopathology shows basal layer hyperpigmentation and DOPA positive melanocytes with no pigment incontinence.
White sponge nevus (Cannon disease)
It is an autosomal dominant genodermatosis affecting oral mucosa, that commonly manifests as bilaterally symmetrical, thickened white, corrugated or velvety, diffuse plaques, predominantly affecting the buccal mucosa. it is asymptomatic and benign so requires no treatment.
The genes responsible are those involved in production of cytokeratins 4 and 13, found in the spinous layers of the oral mucosa. The affected mucosa appears folded with a soft or spongy texture and a peculiar white opalescent hue with diffuse and blending margins of WSN (unlike in leukoplakia that has sharp margins)
Histopathology shows prominent hyperparakeratosis and marked acanthosis with clearing of the cytoplasm of the cells (washed appearance) in the spinous layer. An eosinophilic perinuclear condensation of the cells is seen in the superficial layers of the epidermis, which are tangled masses of keratin tonofilaments (ultrastructural finding).
Hermansky-Pudlak syndrome
Hermansky Pudlak syndrome is a disorder of melanosome biogenesis, most of the cases have mutations in genes that encode components of the biogenesis of lysosome-related organelles complexes 1–3. Patients present with pigmentary dilution of the skin, hair, and eyes. Systemic manifestations due to organelle dysfunction include a bleeding tendency as well as interstitial pulmonary fibrosis and granulomatous colitis secondary to ceroid lipofuscin (similar to leprosy patients treated with clofazimine who can have ceroid-lipofuscin granules in intestine) accumulation within lysosomes. Granulomatous plaques and “knife-cut” ulcers of the vulva, intertriginous areas, and peristomal skin similar to cutaneous Crohn disease have also been described. Pulmonary fibrosis and recurrent infections can be fatal sometimes.
Dermatitis artefacta
The term “artifact” is derived from the Latin words ars (art, handicraft) and facere (to make). Dermatitis artefacta is a frequently unrecognized clinical condition associated with self‐harming behaviour, in which unconscious manipulation causes skin lesions. However, artifacts most commonly involve the skin due to its easy accessibility and the demonstrative character of skin lesions. Depending on the type of injury and the duration of the disease, there may be a variety of histological patterns, some of which mimic other skin disorders. Hence, it is crucial that the clinician informs the dermatopathologist about this diagnostic suspicion (based on history or clinical findings) when sending in biopsy specimens.
In general, findings that should prompt consideration of the diagnosis of dermatitis artefacta include prominent epidermal damage / mummified epidermis due to necrosis, multinucleated keratinocytes or deformed keratinocytic nuclei, as well as an inadequately mild inflammatory infiltrate in early lesions. Absence of the stratum corneum without any substantial inflammatory reaction may also be suggestive of a factitious cause. Other findings include rupture of collagen fibers, multinucleate keratinocytes without bright gray‐blue nuclei with marginalized chromatin (as in the case of HSV infections). Trauma can histologically present with ruptured fat cells, degeneration of adipocytes and hemorrhage. Subsequently, there is a predominance of histiocytes, hemosiderophages, and fibroblasts; eventually leading to fibrosis.
Reference: Tittelbach J, Peckruhn M, Elsner P. Histopathological patterns in dermatitis artefacta. J Dtsch Dermatol Ges 2018;16:559-64.
Hyperkeratosis lenticularis perstans (Flegel's disease)
Hyperkeratosis lenticularis perstans is a rare dermatosis, first described by a German Dermatologist Heinz Flegel in 1958. It is characterized by the presence of flat keratotic papules on the lower legs and dorsa of the feet. It is a disease of the older adults, but it can be seen occasionally in younger persons.
Clinically, it presents with red/brown non‐follicular keratotic papules measuring 1–5 mm in diameter. If the scale is removed, the site is red and may have bleeding points.
Histopathology shows greatly thickened, compact, strongly eosinophilic horny layer standing out in sharp contrast to the less heavily stained basket-weave keratin of the uninvolved epidermis. The underlying stratum malpighii is flattened with thin or absent granular layer. Parakeratosis and epidermal atrophy may be seen occasionally. A lymphoid infiltrate with occasional histiocytes in a bandlike pattern in the papillary dermis is seen close to the epidermis. The lateral edge of the lesion demonstrates abrupt hyperkeratosis and adjacent epidermal atrophy and acanthosis. The lymphocytes, often have nuclei with deep infoldings, resemblingSézary cells.
Electron microscopic studies have demonstrated a lack or paucity of Odland bodies in the stratum granulosum, suggesting a possible mechanism for localized hyperkeratosis.
Acrodermatitis enteropathica
Acrodermatitis enteropathica is an autosomal recessive disorder caused by a mutation in the intestinal zinc transporter gene, SLC39A4, found on chromosome 8q24.3. It manifests in infants as they are weaned from breastfeeding. Infants are often described as listless and apathetic.
The classic clinical triad of acrodermatitis enteropathica is diarrhoea, alopecia and a periorificial and acral cutaneous eruption. The perioral eruption usually spares the upper lip, giving it a ‘U‐shaped’ or ‘horseshoe‐shaped’ appearance. Hair is dry and brittle, and large areas of alopecia may arise. Other cutaneous findings include angular cheilitis, paronychia, delayed wound healing and vitiligo‐like hypopigmentation.
Histopathology shows loss of granular layer, replaced by clear cells and focal parakeratosis. Later lesions show more psoriasiform hyperplasia, confluent parakeratosis and pallor of upper part of epidermis.
Treatment includes daily supplementation of 3mg/kg day elemental zinc. Resolution of symptoms starts occurring within 2-3 days of initiating treatment
Rosai-Dorfman disease/ sinus histiocytosis with massive lymphadenopathy
This non-langerhan cell histiocytosis is a rare disorder characterized by proliferation and accumulation of histiocytes in the lymph nodes and lymphatic channels (sinus histiocytosis). It may be caused by infectious agents (Epstein-Barr virus, human herpesvirus six, parvovirus B19, herpes simplex virus, Brucella, Klebsiella rhinoscleromatis and Nocardia), immunodeficiency, or autoimmunity. Clinically, it manifests with firm, red to red-brown or xanthomatous macules, papules, nodules or plaques with satellite lesions that are slow growing and frequently multifocal and clustered.
Dermal infiltrate of histiocytes with large vesicular nucleus and the cytoplasm (‘oyster’) containing different types of bone marrow cells, such as lymphocytes or neutrophils (‘pearls’) within it (emperipolesis). There is a background infiltrate of mature lymphocytes and plasma cells. Immunohistochemical staining shows S-100 positive, CD68 positive, and CD1a negative. It is usually self-limited.
Multinucleated giant cell angiohistiocytoma
Multinucleated giant cell angiohistiocytoma is a rare benign disorder first described by Smith and Wilson Jones in 1985. Women aged 40 years and above are predominantly affected (female: male 5:1). It is postulated to be due to a reactive change, possibly due to vascular injury. Female hormones have also been implicated.
Clinically, it presents with firm, grouped, dome-shaped red to purple colored papules with a predilection for extremities.
Histologically, there is a proliferation of small capillaries and venules in the superficial and mid dermis and thickened collagen bundles. Perifollicular and perivascular cell infiltrate, composed of histiocytes, lymphocytes, and occasional plasma cells and neutrophils are seen. Scattered angulated, bizarre multinucleated giant cells with basophilic cytoplasm are characteristically seen that stain positive with vimentin and factor XIII. These cells stain negatively for CD 31, 34 and S-100.
It is generally benign but tends to increase in size with time.
Pityriasis rosea
It is characterized by an eczematoid reaction pattern called the “Unna sign” and an undulating appearance of the epidermis. The mounds of parakeratosis are partly lifted from the epidermis to give the tilted appearance, known as the “teapot lid sign”. Also there can be dyskeratotic cells at all levels, especially in the herald patch.
The papillary dermis shows edema and RBC extravasation extending to epidermis, also known as the Sabouraud sign. All these features differentiate pityriasis rosea from its clinical mimics such as guttate psoriasis.
Grover’s disease (transient acantholytic dermatosis)
Grover’s disease was first reported by Dr. Ralph Grover, an American dermatologist, in 1970. It is characterized by transient, self-limited, intensely itchy, papulovesicular or papular rash usually involving the upper trunk in elderly men. It begins as a sudden onset of small tiny, discrete papules and vesicles that quickly form crusts and keratotic erosions. This itchy rash is frequently exacerbated by heat, sweating, and UV light. Grover’s disease can coexist with various other dermatoses like eczema, psoriasis, and malignancies. Histologically, acantholysis seen in Grover’s disease occurs in a variety of patterns: Darier's disease-like, Hailey Hailey disease-like, pemphigus vulgaris-like, and spongiotic. Other early microscopic findings include elongation of rete ridges, few dyskeratotic cells, mild spongiosis and a dermal infiltrate containing eosinophils. The presence of eosinophils in Grover disease distinguishes it from Darier’s disease. Another histological variant, with acantholysis localized to acrosyringium, has also been reported.
Cowdry (cow+dry) body
Cowdry bodies are intranuclear inclusions seen in viral diseases. These could be either eosinophilic or basophilic. They are named after Edmund Cowdry. These can be seen in herpes simplex virus, varicella zoster virus, cytomegalovirus and other viral infections. The size is highly variable and they appear much larger than they nucleolus. They are traditionally detected by Romanovski staining on air-dried smear (the Tzanck smear). However, these inclusions are best appreciated on Papanicolaou staining after 95% ethanol wet fixation.
Rope+ Collagen(college)= Ropy/ropey Collagen
Ropy collagen indicates thickened bundles of collagen.
It is not a specific diagnosis, however, its presence provides an important diagnostic clue for spindle cell/ pleomorphic lipoma.
Spindle cell/ pleomorphic lipoma is a benign lipomatous tumor which usually involves the subcutaneous plane or superficial soft tissue. The common locations include back of neck, upper back and shoulder. It is a well circumscribed tumor, composed of mature adipocytes and spindle shaped cells, in a variably myxoid stroma. The spindle cells can show variable pleomorphism. Multinucleated/ floret giant cells can be rarely observed. The background shows presence of ropy collagen. By immunohistochemistry, the spindle cells show CD34 expression, while the adipocytes show S100 expression. They have a favourable prognosis.