Answer to Image of the Month January 2014
Submitted by Mani Makhija, Hemamalini Aiyer
Lafora disease
Lafora bodies are PAS positive and diastase resistant inclusion bodies, which are age related, insoluble, abnormal glycogen named polyglucosan. Polyglucosan accumulates in tissue with age but in Lafora disease their numbers are increased tremendously even in the second decade of life, leading to a fatal neurodegenerative disease.
A skin biopsy is submitted to confirm the clinical diagnosis of Lafora disease in a case of progressive myoclonic epilepsy. There are usually no skin lesions and a biopsy from normal appearing skin of the axilla is taken to sample the largest number of apocrine ducts (where inclusions are deposited preferentially). H&E stained sections are unremarkable and PAS stain is required to detect the inclusions. The inclusions are carbohydrates and are seen as PAS-positive diastase-resistant inclusions in the cytoplasm of the apocrine and eccrine ducts. The inclusions are of a size that is nearly comparable to the nuclei of the sweat duct cells (see image below). On ultrastructural examination, they are seen as non-membrane bound, round to oval bodies composed of fine filamentous material, darkly staining granules and vacuoles.
Lafora’s disease is characterized by progressive myoclonic epilepsy and rapid decline in cognition. Other differential diagnoses for the clinical presentation include mitochondrial myopathy, Unverricht-Lundborg disease, ragged red fibers disease, neuronal ceroid lipofuscinoses and type I sialidosis. Skin biopsy is a simple investigation that helps definitively identify one of the causes of this neurological syndrome.
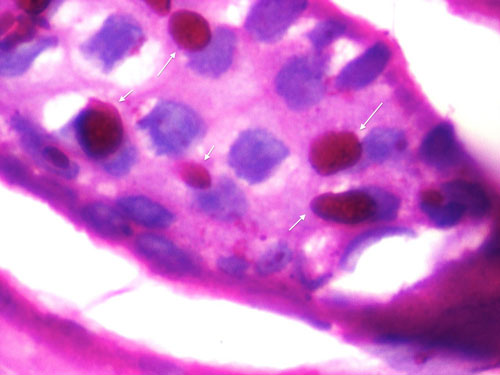 White arrows point to PAS-positive Lafora bodies within a sweat duct (PAS, oil immersion)
White arrows point to PAS-positive Lafora bodies within a sweat duct (PAS, oil immersion)